What the child and infant mortality statistics cover, how we produce them, and their quality and comparability. Includes definitions and latest, past and upcoming changes.
We produce annual statistics on child and infant mortality in England and Wales. These include characteristics of babies and parents, and analysis of risk factors in relation to deaths. We produce these by linking information from birth registrations, birth notifications, and death registrations in England and Wales.
It is a legal requirement to register births and deaths (and for healthcare providers to submit birth notifications) within a certain time and with correct information. This means the data is generally complete.
We and the registrars carry out thorough validation and quality assurance checks on the data to ensure our statistics are as accurate as possible.
We updated this guide on 8 April 2025. Important changes to quality and methods include:
updating the name of the child mortality (death cohort) tables to “child and infant mortality (by year of death)” for deaths in or after 2023
updating the name of the infant mortality (birth cohort) tables to “infant mortality before their first birthday (by year of birth)” for births in or after 2022
An infant death (a death that occurs within a year of birth) can occur in the same calendar year as the birth, or the subsequent calendar year.
Some users need deaths information for a group of infants born in a particular calendar year, while some need it for a group of infants that died in a particular calendar year.
The child and infant mortality (by year of death): 2023 dataset contains information on all infants that died in 2023 before their first birthday, that were born in 2022 or 2023.
The infant mortality before their first birthday (by year of birth): 2022 dataset contains information on all infants that were born in 2022, that died in either 2022 or 2023 before their first birthday.
Breakdowns in the datasets
Both datasets include breakdown by characteristics of the baby and mother, and age at death. These allow us to make useful comparisons.
Characteristics categories
Baby’s birth weight
Baby’s gestational age (how long a baby has spent developing inside the womb between conception and birth)
Office for National Statistics (ONS) cause of death group
Mother’s age at birth of child
Mother’s country of birth
Mother’s marital status
Mother’s number of previous children
Place of delivery
Parents’ socio-economic status National Statistics Socio-economic Classification (NS-SEC) (as defined by occupation)
These categories allow us to compare death rates – for example, between younger and older mothers, and between babies with low and normal birth weights.
How place of delivery information differs between the two datasets
We use different classifications for place of delivery between the two datasets.
For the child and infant mortality (by year of death) dataset, we get place of delivery information from birth registrations and birth notifications. We include breakdowns by the following places of delivery:
hospitals
other healthcare establishments
at home
elsewhere
For the infant mortality before their first birthday (by year of birth) dataset, we only get place of delivery information from birth notifications. We include breakdowns by the following places of delivery:
NHS hospital – delivery facilities associated with midwife ward
NHS hospital – delivery facilities associated with consultant ward
NHS hospital – delivery facilities associated with consultant, GP or midwife ward inclusive of any combination
NHS hospital – ward with no delivery facilities
private hospital
other hospital or institution
domestic address
unknown
Age at death categories
Child (only included in the by year of death dataset): those aged between 1 and 15 years old
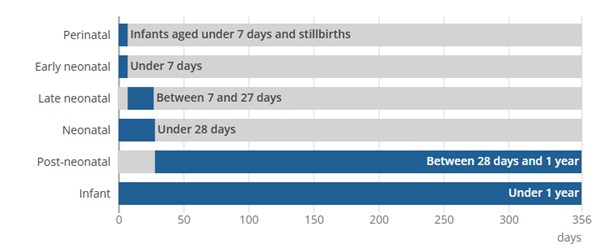
Infant: those aged under 1 year old
Post-neonatal: infants aged under 28 days and 1 year
Neonatal: infants aged under 28 days
Late neonatal: infants aged between 7 and 27 days
Early neonatal: infants aged under 7 days
Stillbirth: those born after 24 or more weeks' gestation that did not breathe or show signs of life during or after delivery
Perinatal: those aged under 7 days and stillbirths
Figure 1
Age at death categories
England and Wales
Source - Child and infant mortality quality and methods guide, from the Office for National Statistics
those still-born before 24 weeks’ gestation – we categorise these as miscarriages
births and deaths of England and Wales residents that occur and are registered outside of England and Wales
Sub-divisional breakdowns (for regions, counties, metropolitan counties, and local authorities) also exclude births and deaths of non-England and Wales residents registered in England and Wales. However, these are included for the total England and Wales figures.
Where the data come from
Birth registrations
A parent must register a birth with a registar within 42 days.
Birth registrations include information about:
the birth and the baby – such as the date, sex, and whether one or more babies are born (known as single or multiple birth)
the biological mother – such as her usual residence, and her age at the time of the birth
the second parent if the parents are married or in a civil partnership, or if the second parent is present at the registration (known as joint registration)
Birth notifications
Midwifery staff present at the birth must submit a birth notification within 36 hours:
directly onto the Personal Demographics Service (PDS) if using a PDS-compliant system
through the National Care Records Service (NCRS) if using a non-PDS compliant system (which in turn updates the PDS)
Once the baby's birth notification is available, the PDS notifies us.
A birth notification includes information that is not included on the birth registration, such as gestation length and the baby’s ethnicity.
Death registrations
A death must be registered by “the informant” (a relative, someone present at the death, the occupier of or an official from the public building where the death occurred, or the person arranging the funeral) within five days of it occurring.
the death – such as cause of death, when the deceased was last seen alive, and whether a post-mortem was carried out
the deceased – such as their sex, usual residence, place of birth, and date of birth
How we produce the statistics
Linking death registrations with birth registrations
We link death registrations with corresponding birth registrations. This allows us to get more social and biological information about the baby and parents than we could from death registrations alone.
Linking death registrations with birth notifications
Where possible, we’ve also linked death registrations with corresponding birth notifications back to 2007 – the earliest year we can apply this type of linkage. This allows us to get more information about the baby, such as gestational
age and ethnicity, than we could from death registrations and birth registrations alone.
Why linking a death with gestational age and ethnicity information is important
Having a low gestational age and being from a Black or Asian ethnic group are two of the main risk factors associated with deaths in the perinatal (stillbirths and early neonatal) period. Linking these helps to provide better analysis of the relationship between gestational age and ethnic group with deaths.
Linking birth notifications with birth registrations
The registrar links birth notifications with birth registrations, which creates a unique sequence number. We use this number to carry out our own re-linkage.
If the registrar has not been able to link a birth registration and birth notification (meaning the unique sequence number is not available), we use probabilistic linkage. This means we link birth registrations with birth notifications
based on the likelihood of them being for the same baby.
When we extract the data and carry out linkage for child and infant mortality (by year of death) dataset
We extract the total number of deaths occurring in a calendar year (known as the “data year” – for example, 2023) from the deaths registrations database. We do this approximately 9 to 10 months after the end of the data year to allow for late registrations.
We do not publish the small number of registrations registered after we extract the data. This is an appropriate balance between accuracy and timeliness.
We then link these deaths with birth registrations and birth notifications.
We usually cannot link around 3% of deaths (9.5% for the 2020 data year because of the coronavirus (COVID-19) pandemic – read more in Strengths and limitations). The main reasons are not being able to find a birth record, or the birth was registered outside of England and Wales.
When we extract the data and carry out linkage for the infant mortality before their first birthday (by year of birth) dataset
We extract the total number of births occurring in a calendar year (known as the “data year” – for example, 2022) from the birth registrations database and birth notifications database. We do this approximately six to seven months after the end of the data year and then link the two.
Next, we extract the infant deaths occurring in the same year as the birth, and in the following year (for example, 2022 and 2023, respectively). We extract data for both years because an infant born near the start of the data year may die during that year before their first birthday, and an infant born near the end of the data year may die in the following year before their first birthday. We do this 10 to 11 months and 22 to 23 months after the end of the data year, respectively.
This means that the infant mortality before their first birthday (by year of birth) dataset is less timely than the child and infant mortality (by year of death) dataset. However, this time lag allows us to provide additional analysis.
We then link the birth and death occurrences to decipher how many infants that were born in a certain data year died before their first birthday.
Quality of the statistics
Statistical accreditation
These accredited official statistics were independently reviewed by the Office for Statistics Regulation in February 2013. They comply with the standards of trustworthiness, quality and value in the Code of Practice for Statistics
and should be labelled "accredited official statistics”.
How we quality assure the data and statistics
The registrar carries out validation checks when a birth or death is registered.
We carry out validation and consistency checks when we extract births and deaths data from the databases – this eliminates any errors made in the supply and recording of birth and death registrations.
We carry out more frequent and thorough checks on registrations with extreme values for the main variables (such as age of mother and father), as these have a greater impact on the statistics.
If we spot a registration that doesn’t look right, we raise it with the General Register Office (GRO) for additional verification – we usually only need to do this for a small number of registrations per month.
Strengths and limitations
Strengths
Producing two datasets means we provide breakdowns of child and infant mortality by year of death, and infant mortality before their first birthday by year of birth, maximising the statistics’ coverage and usage.
The number of birth and death occurrences provided by birth registrations, birth notifications, and death registrations are generally complete and accurate; it is a legal requirement to submit these
with the correct information and within a certain time period, and both we and registrars carry out validation checks (read more in
How we quality assure the data).
Limitations
There were delays to birth
registrations in 2020 and 2021 because of the coronavirus (COVID-19) pandemic, which meant we had to extract births data later than usual; this affected the timeliness of the statistics, but meant we could
include more late registrations and improve the accuracy.
The pandemic also affected linkage between birth registrations, birth notifications, and death registrations for 2020 and 2021; in 2020, we could not link 9.5% of child and infant deaths, compared with around 3% for 2007 to 2009, and 2022.
European Statistical System Quality Dimensions
The Office for National Statistics (ONS) has developed
Guidelines
for measuring statistical quality based on the five European Statistical System (ESS) Quality Dimensions. These are:
relevance
accuracy and reliability
timelessness and punctuality
comparability and coherence
accessibility and clarity
We have integrated these considerations into the guide.
Changes and their effects on comparability over time
Over the years, we have changed how we produce child and infant mortality statistics. Sometimes this is to improve the statistics, and sometimes it is because of external changes (such as software advancements, changes to policy, or changes to legal definitions).
Changes can sometimes affect comparability of the statistics over time.
Latest changes
Dataset name changes
On 8 April 2025, we changed the name of the child mortality (death cohort) tables to “child and infant mortality (by year of death)”. This explains more clearly what we mean by “death cohort” (that the statistics are organised by year of death), and that the dataset includes statistics for infants as well as children. This name change applies to the 2023 data year onwards.
On 8 April 2025, we also changed the name of the infant mortality (birth cohort) tables to “infant mortality before their first birthday (by year of birth)”. This explains more clearly what we mean by “birth cohort” (that the statistics are organised by year of birth), and that the dataset is specifically about babies that die before their first birthday. This name change applies to the 2022 data year onwards.
The statistics themselves have not changed, so this does not affect comparability over time.
Past changes
These changes are ordered by date, with the most recent first.
Definition of a stillbirth
From the 2021 data year, we stopped classifying live births at 23 and 24 weeks as stillbirths. This had no significant effect on the stillbirth rate, so does not affect comparability over time.
On 1 October 1992, the definition of a stillbirth changed from 28 or more weeks’ gestation to 24 or more weeks’ gestation (Still-Birth (Definition) Act 1992). This means our statistics on stillbirths from the 1993 data year are not directly comparable with previous releases.
Software we use to code death registrations
We have used different softwares to code cause of death over the years.
From the 2021 data year, we updated our software from to Multicausal and Unicausal Selection Engine (MUSE) 5.5 to MUSE 5.8. In line with this, we updated the hierarchical classification system we use to classify ONS cause of death groups for stillbirths and neonatal deaths for statistics.
This means ONS cause of death groups from the 2021 data year onwards are not directly comparable with 2014 to 2020.
From the 2018 data year, we updated our software from Iris to MUSE 5.5. MUSE 5.5 increased the automation of coding and operated based on internationally agreed decision tables to reflect the ICD-10.
This change slightly reduced comparability with previous releases, but increased accuracy in coding causes of death.
On 1 January 2014, we updated our software from Medical Mortality Data Software (MMDS) to Iris. Iris incorporated official updates to the ICD-10 approved by the WHO, helping to improve international comparability.
For stillbirths and neonatal deaths, Iris coded maternal condition mentioned on the death certificate to chapter XVI (certain conditions originating in the perinatal period) rather than chapter XV (pregnancy, childbirth and the puerperium).
These changes limited the comparability of the “antepartum infections” and “infections” cause of death groups from the 2013 data year with previous releases.
Ethnic groupings
In 2021, we updated baby ethnic groups to better align with the groups used in Census 2021 back to the 2019 data year, meaning they are not directly comparable with previous releases.
In 2020, we introduced three new tables in the child and infant death (by year of death) dataset on the number and rates of live births, stillbirths, and infant mortality by ethnicity. These were previously available in our Births and deaths by ethnicity dataset for 2007 to 2019 .
This does not affect comparability of the statistics over time.
How we present unlinked death
We have made several changes to how we present unlinked deaths (deaths that could not be linked to a birth) over the years.
For the 2020 data year, we created a separate category for unlinked deaths.
For the 2019 data year, we included unlinked deaths in all tables in the by year of death dataset. We included them in a “not stated” category in tables that analysed birth registration variables, and presented them separately in tables that analysed death rates for linked deaths.
Before this, we had left unlinked deaths out of some of the tables completely.
Geographic boundaries
Since the 2017 data year, we’ve used the latest geographic boundaries for sub-divisional breakdowns.
Any changes to geographic boundaries can affect the comparability of sub-divisional breakdowns over time. Find specific changes in our Data sources guide to mortality statistics.
When we extract data for the infant mortality before their first birthday (by year of birth) dataset
From the 2015 data year, we began extracting death registrations 10 to 11 months and 22 to 23 months after the end of the data year, respectively.
The change meant we captured 5% to 6% more late registrations, and that statistics from the 2015 data year are not comparable with previous releases.
Information collected about previous children on birth registrations
From May 2012, birth registrations started including the number of previous live births and stillbirths all mothers had had, rather than just those married mothers had had with the current or former husband. This change came about because of amendments to the Population (Statistics) Act 1938.
This simplified the question and led to improved accuracy in responses, but means statistics from the 2014 data year onwards are not directly comparable with previous releases.
Read more about the impact of this change on our birth statistics:
In 2012, we started categorising the statistics by the most advantaged parent’s socio-economic classification (a “household-level classification”). Previously, we had automatically categorised the statistics based on the father. This was because many mothers did not have a paid occupation or chose not to state their occupational details on the birth registration.
In 2011, we rebased the NS-SEC on the new Standard Occupational Classification (SOC 2010) to categorise socio-economic class. This change meant classifications were based on employment conditions instead of skills to more accurately describe modern occupations.
Both of these changes means statistics from the 2012 data year onwards are not directly comparable with previous releases.
From the 2010 data year, we categorise births registered to same-sex couples:
in civil partnerships as "marital births"
outside of civil partnerships as "non-marital births"
The numbers of births registered to same sex-couples is relatively small, so this change has a negligible effect on comparability over time.
We include footnotes in the datasets stating the number of births registered to same-sex couples included in the numbers.
Statistical classifications of disease systems we use to we code cause of death
We have used different revisions of the International Statistical Classification of Diseases (ICD) to code cause of death over the years.
From the 2009 data year, we switched from using ICD-10 v2001.2 to ICD-10 v2010.
From the 2000 data year, we switched to using the International Statistical Classification of Diseases 10th revision (ICD-10) to code causes of death, based on the recommendation of the WHO. This replaced the ICD-9, which we had used since 1979.
These changes limited comparability with previous releases, but resulted in:
diseases and groups of conditions that reflected more up-to-date medical knowledge
improved selection of the underlying cause of death
improved international comparability
Death registration certificates
In 1986, England and Wales introduced new certificates for registering neonatal deaths (infants that died aged under 28 days) and stillbirths in line with a recommendation from the World Health Organization’s (WHO).
These are different to standard death certificates – they do not assign a single underlying cause of death, and instead give certifiers more flexibility to report on multiple relevant diseases in both the infant and the mother.
This meant we could no longer directly compare a single underlying cause of death for neonatal deaths and stillbirths with postneonatal deaths (infants that died aged between 28 days and 1 year).
This allows us to directly compare stillbirths and neonatal deaths with postneonatal deaths, despite the differences in registration.
Upcoming changes
We currently have no plans to change the methods in the near future.
Comparability and coherence with other statistics producers
Mothers and Babies: Reducing Risk through Audits and Confidential Enquiries across the UK
Mothers and Babies: Reducing Risk through Audits and Confidential Enquiries across the UK's (MBRRACE-UK) Infant mortality statistics are not comparable with ours because of the following differences.
ONS
MBRRACE-UK
Includes deaths of children up to 15 years
Includes infant deaths only
Includes all live-born babies, including those born before 24 weeks
Excludes live-born babies born before 24 weeks
Includes stillbirths from 24 weeks' gestation in line with the legal definition
Includes stillbirths from 22 weeks' gestation
Northern Ireland Statistics and Research Agency
Northern Ireland Statistics and Research Agency's (NISRA) Child and infant mortality statistics are not comparable with ours because of following differences.
ONS
NISRA
Based on date of death occurrence – gives a more accurate representation of deaths in a given year and helps track trends over time
Based on date of death registration – reduces the delay in producing statistics, but result in less complete statistics because late registrations are not captured
Based on date of death occurrence – gives a more accurate representation of deaths in a given year and helps track trends over time
Based on date of death registration – delays are shorter in Scotland, so little difference between death occurrence and registration dates
Users and uses of these statistics
A range of organisations and government departments use our child and infant deaths statistics to inform services and policies, and ensure targets are met. For example:
the Department of Health and Social Care (DHSC) includes our statistics in their
child and maternal health profiles; local organisations
use these to create reports, tools, and other resources to plan services based on what their area needs
our statistics are used to monitor the NHS’s, the Welsh Government’s and the UK Government’s progress towards targets outlined in the
NHS outcomes framework, such as
reducing deaths in babies and young children
the United Nations (UN) Statistics Division uses our statistics alongside statistics from Scotland and Northern Ireland to monitor the UK’s progress towards global indicators, as part of the UN’s
Sustainable Development Goals
Other users include academics, researchers, charities, and the media.
Definitions
For definitions of how we categories different ages at death, go to
Age at death categories.
Linkage
The matching of death registration records to their corresponding birth registration record and/or birth notification record, and birth registration records to their corresponding birth notification record.
Occurrences
The number of:
deaths according to the date on which the death occurred
births according to the date on which the birth occurred
Registrations
The number of deaths according to the date on which the deaths were registered, and the number of births according to the date on which the births were registered.
Underlying cause of death
“The disease or injury which initiated the train of morbid events leading directly to death, or the circumstances of the accident or violence which produced the fatal injury”, in accordance with the rules of the International Classification
of Diseases (excludes deaths that occurred under age 28 days).
Annual statistics on births and infant deaths based on babies born in a calendar year that died before their first birthday linked to their corresponding birth notification and their corresponding death registration.
Supporting information for mortality statistics, which present figures on deaths registered in England and Wales in a specific week, month, quarter or year.
Supporting information for birth statistics, which present figures on births that occur and are then registered in England and Wales. Figures are based on information collected at birth registration.